Without a full length mirror around, do you remember that you are disabled? I’ve been a quadriplegic for years now, but the shock of seeing myself is a never-ending surprise.
I give talks now and then about what it means to live with an imperfect body. I spent ten years making art about it, before I lost the use of my hands. I think about the imperfect body A LOT. Illness and disability are a huge part of my life. But still, believe it or not, I don’t think of myself as disabled.
Yesterday I watched a video of a recent discussion I had with Ted Meyer, and Dr. Amezcua with the medical students and faculty of the Keck School of Medicine of USC. I had prepared for this talk for several weeks; I was speaking about using art as a way of communicating, a subject I am passionate about and comfortable with. That day, I felt happy, empowered and confident.
But watching the video of that day, I saw something very different from what I had experienced. My body was slumped, with horrible posture. My hands were frozen, wrapped around my body. Listening to the audio, I can hear that I’m having trouble finding the right words. My voice is weak.
Watching this, I am absolutely shocked. I feel bad for the woman in the video. God, she is really disabled, I think to myself. She does not look powerful. She literally grew smaller and smaller over the course of the one hour talk, her core muscles unable to support her in her wheelchair.
I guess that’s how people see me? I begin to cry.
This cognitive dissonance weaves its way into other parts of my life, and it isn’t always a feeling of shock. It can be funny. For example a few months ago I ordered a ridiculously expensive silk scarf online, with a plan in mind. It was so colorful and vibrant, I thought people would focus on the scarf and see my personality, my fashion sense. I wanted people to find me attractive.
When the scarf came in the mail, I was dying to try it on. I asked my caregiver to drape it just so (it took some time to get it right) and when my husband came into the room, I asked him, “Honey, what do you think? It was a bit expensive but… don’t you think this scarf makes me look less disabled?”
He hemmed and hawed a bit and then bashfully gave me an honest answer: “The scarf doesn’t make you look less disabled, Elizabeth.” He looked at the price tag and nearly fell over. “I would return it.” We both laughed.
My husband and I have been together many years. I don’t want you to think his reaction was unkind. He’s just honest. He’s looking at me in my 400 lb. wheelchair, his wife who he sees day in and day out. He navigates the wheelchair, cleans my glasses…And so, we have our special version of, “Honey, do these jeans make my butt look big?” It’s an unfair question.
The scarf incident didn’t really hit me the same way as the video. I brushed it off — “I think this scarf looks AMAZING.” I kept it, wore it and felt great.
But I am stuck on how it felt to watch myself in that hour long video. My view of myself made me feel small, and made me cry. I don’t usually worry about my arms, my clenched, claw-like hands.
I’m struggling with this. I don’t have a snappy ending or a moral to this story. How can I maintain a feeling that I am powerful, doing meaningful work, when I suddenly see a person in the mirror who I do not recognize? I’m stuck between two worlds. For my internal sense of self, my beautiful scarf is alluring. But the reality is, I don’t think people will even notice the damn scarf. Instead, a focus on the wheelchair, and the stiff, frozen arms.
I have taken somewhat of a hiatus from my blog, and from social media in general, because the last few months I have been in an all-consuming battle with myself to craft my story and present it coherently for a Ted X Stanford talk about learning to embrace and even celebrate the imperfect brain.
Well, the talk was a few weeks ago and I survived it! It was the most nervous I’ve ever meet in my life. Baring your soul on stage is nothing like arguing a case in front of a courtroom…
I have resurfaced from my Ted x talk madness to share the story of an incredible event put on by my friend Ted Meyer, an artist who portrays the “beauty and humor of physicality while exploring narratives of the human condition.” He is a resident artist and curator at USC Keck School of Medicine this year, and has successfully curated a show that celebrates the collaboration between art and science in a way that is unique, honoring both art and science.
In Artist and Researcher, Meyer paired 14 USC medical researchers with 14 local artists. Each grouping’s work either intersects in some obvious way (such as artist Susan Trachman who lives with MS, and researcher Leslie J. Tarlow who researches MS) or in a more metaphorical, elusive way (such as artist Cybele Rowe, who is a largescale sculptor interested in form and Tiffany Chow, who is dedicated to finding the cause of Alzheimer’s) Meyer essentially opened the door for conversation, set the table, and let the dialogue begin.
Artwork by Susan Trachman
Artist Zeina Baltagi, researcher Amy Firth
I watched the video of the opening, where the artist / researcher pairings were interviewed about the process of creating together. What struck me most was each collaborator was as an equal – there was no elevation of the science, no pretensions around the art. It was not multidisciplinary, but interdisciplinary, with all the connotations that an intersection brings. To roads converging, two paths becoming one, and the cross-section where they overlap becomes a rich meeting place for community members to stop, rest, reflect, and re-orient.
I particularly liked how researchers discussed their reactions to the artist’s studio, and how they found inspiration and connections to their research. As an artist, I have always found profound inspiration within medical data, neurotechnology, and the field of science in general. When scientists find inspiration in my work, I feel I am creating something universal for people of all disciplines to take something from. To imagine a researcher in my studio delving into my images, sketches, and process, and to imagine them discovering a spark that brings them further in their own field… that is something incredible.
Ted Meyer and the team at USC has done something amazing; not only noticing the overlapping of art and science and curating a show that depicts that – but also making space for a creative laboratory where art and science to play off of one another, where the artist-researchers had space and time to form meaningful relationships with one another. Thank you to all the scientists and artists who continue to collaborate and enrich what it means to be human!
The opening night of Artist & Researcher was fortunately caught on film; to watch scientist-artist interviews, see some of the work, and learn more about the show, please click here to watch!
Scientist-Artist pairings:
Lilyana Amezcua, MD, MS + Kerry Kugelman
Tiffany Chow, MD + Cybele Rowe
Vinay Duddalwar, MD, FRCR + Michael McCall
Amy Firth, PhD + Zeina Baltagi
Laurel M. Fisher, PhD + LuAnn Roberto
Gino K. In, MD, MPH + Olesya Volk
Elina Kari, MD + Jamie Perlman, MA
Peter Kuhn, PhD + Leah Shane Dixon
Francesca V. Mariani, PhD + Andrea Bogdan
Andy McMahon, PhD, FRS + Barbara Kolo
Marilena Melas, MSc + Shula Singer Arbel
Michael E. Selsted, MD, PhD + David Lovejoy
Soma Sahai-Srivastava, MD + Qathryn Brehm
Leslie J. Tarlow, MSN, RN, GNP-BC, MSCN + Susan Trachman
Treating people, not illnesses: storytelling is at the heart of “holistic”
As we have shaped our ideas about how health care can be transformed into a more human, holistic experience, we’ve explored the impact of visual art, human-centered design, and sound. Through all this, storytelling has been a central theme: use art to make stories visible. Implement design that integrates storytelling with ease. Transform sounds to make space for an authentic, empowering narrative.
All of this aims to humanize the experience of illness within a flawed system.
As we’ve connected with others who envision a more human health care system, we’ve discovered the disarming and simultaneously grounding effect of humor.
Does humor have a role in the narrative of chronic illness?
Can living with chronic illness be humorous?
If the answer to this set of questions is a yes (and I think it is), what does our need to laugh at ourselves – to find humor in our own imperfections – teach us about being human?
People who humanize health care use a dynamic, evolving toolkit. Patient-centered design, telehealth, storytelling initiatives, and inclusive conferences are like screwdrivers, wrenches, and hammers. They are the tools that build a better health care system.
Humor, however, holds a special magic. It makes the heavy things in life light. Laughing at oursevles, discovering new parts of our selves, and most importantly reinforcing our ability to feel a release.
Does humor have a role in the narrative of chronic illness?
I begin this blog with an interview with Ann Feehan, a member of BATS Improv, a theatre company that “cultivates and innovates the craft of improvised theatre through engaging, playful, creative performance and training.” Her work with improvisational theatre includes working alongside people who are dealing with serious illnesses through a program called Laughing Stock. I was inspired to explore the world of comedy and specifically Ann’s work because one of my closest friends who has stage four breast cancer took a class with Ann and absolutely loved it.
What is improvisational theater?
Improvisational theatre isn’t focused specifically on being funny or telling jokes – not in the traditional way. Right off the bat, Ann described improv as “story-based” and “in the moment.” Because “telling stories is a natural human ability,” this means everyone is capable of trying improvisational theatre: a form of performing art that relies on our collective imaginations and our ability to say “YES! And…”
Tell us more about “Laughing Stock.”
Laughing Stock started in the HIV / AIDS community, and over time extended to life threatening illnesses, including hep C and cancer. Laughing Stock is not drama therapy. There is no planned content about what people are going through; participants are invited to talk about whatever they please.
“When people are ill or have a disability, that’s how everybody sees them: [improv] is a sort of a vacation.”
The Laughing Stock team offers drop in classes, where some people come regularly, others are more sporadic. People who attend class and are interested in performing participate in shows and demos with organizations such as UCSF, a cancer center in Concord, CA, and the Marin AIDS Project.
4 reasons improv is important to people living will illness:
1. YES is an option
“Improv is important because it’s easy to feel powerless. [Illness can] derail you. Improv helps people to say yes to things. When you are sick, you are forced to accept things you don’t like, treatments you have to take – [improv reveals] there are other choices you can make, such as accepting help from others.”
2. A change of perspective
“In improv we play lots of different “statuses.” You might be the king, you may be a homeless person… You can expand your range of what you are feeling comfortable performing, but also what you are comfortable expressing. It gives you permission to express all the parts of your self. People realize that a part of them they didn’t think was important is worth exploring, expressing and developing.”
3. Shared community
The shared community and exchanges between people at Laughing Stock reveal that there are still opportunities in life, even if one lives with an illness. “It’s easy to feel like no one understands what your thinking, but then [during rehearsal, you try something] – everybody saw it, everybody gets it.” This unifying moment is transforming.
4. Laughter over pain
“Improvisational work starts with ice breakers: when people laugh together it builds a lot of trust. It’s hard to feel pain and laughter at the same time. One participant with cancer [who had been in extreme pain throughout the week] mentioned that they hadn’t felt pain the entire performance.” Improv allows us to release tension and feel closer to others.
Not a patient; a person. A hilarious person.
Can humor empower those of us living with illness?
Laughing at oneself with the collective audience chuckling along as opposed to being the butt of a joke (or worse, a “buzzkill) is an empowering “flip” that parallels the epatient revolution. ePatients are people taking charge of the practical elements of their healthcare via self-advocacy and networking. People who take charge of their mental health, whose philosophies and daily perspectives are in direct resistance to the stigmas associated with illness are some of the best comedians among us.
We have compiled a modest list of comedians within the chronic illness community – focusing specifically on those of us living with Multiple Sclerosis.
Jim Sweeny
“You’re a long time dead…I can either sit around moaning about it now, or just get along with living and just take whatever happens.”
We acknowledge this is a very limited list; please feel free to share in the comment section and add to our portfolio of comedians who are flipping the narrative of illness.
Co-written by lead artist Elizabeth Jameson and co-creator Catherine Monahon
On silence, public spaces, and the potential for art
Introduction by Catherine Monahon, my studio assistant:
There are implicit rules we learn from a young age. For instance, in certain public spaces silence is expected. We are shushed in elevators, trains, and lines. As we grow older, the silence settles and becomes our new norm. We don’t usually strike up conversations with strangers; we do not have the emotional bandwidth, interest, or time. Oftentimes I wonder during my commute to work if anyone else on the train is depressed like me. Homesick like me. Confused about relationships, anxious about work, angry about the news… everyone looks at their phones or out the window, and most of us conform to the silence.
The waiting room of an MS clinic may be one of these spaces — a somewhat public space, full of people, where silence rules. But there is a catch. Here, in a confined space for undetermined amounts of time, wait people of all walks of life with something in common. Here are elders, young people, people of all genders and orientations, various spiritual beliefs, black, brown, white, people with different types of MS, different abilities, and different stages of progression – all united by a diagnosis. United by a diagnosis, but perhaps not by emotion or circumstance.
Within this particular silence, there are a vast array of stories waiting to be told. I believe that when people share stories it is like sharing seeds; enriching our lives, diversifying the environment, and growing something together. If we can break the silence of the waiting room these stories will germinate, creating connections between people and generating resilience as they blossom with the help of art and technology.
And on that note, I turn it back to lead artist, Elizabeth Jameson:
The Baby Chicks Waiting Room Incident of November 2015
In my first blog post, I told the story of my experience exactly one year ago in an MS waiting room. This blog was born in part due to my anger and loneliness in facing a disease which leaves me without the use of my arms and legs. My anger was not because of the disease; my anger was because while I was in that waiting room, I felt diminished. It was not just the silence, but also the video of baby animals that had been left on repeat and the fact that there was no space made to connect with others, no acknowledgment of the invisible emotional life of the waiting room.
I sense a desperate need of every person for something more, something like a sense of community. We are all in it together, sitting in this MS waiting room and experiencing what it means to be human; facing a disease that has no rhyme or reason, and life goes on. But how in the world do we deal with it?
One Year Later
Fast forward a year, to November 2016. I visited the very same waiting room, and I was disheartened again. Barely anything had changed. The only change was the video, which had been amended to include impressionistic imagery and nature scenes in addition to the baby animal sequence. The images were on a continuous loop that was so quick, you couldn’t even take the time to try and engage with the content. After seeing that video, I decided to I want to put my talent and attention to the needs of people who are like me., alone in the journey of chronic progressive disease.
Breaking the silence
During my wait, I surveyed the room, scoping out body language to see if other patients were actually looking at me or even noticing me (I’m hard to miss in my wheelchair). The silence in the waiting room is so pervasive that patients and their loved ones don’t even speak. Medical assistants shuffle through periodically, taking vital signs and introductory information before the patients see their doctors. There are no reading materials except for MS specific literature. I did not see anyone look up at the video I had been triggered by. One woman was on her phone, the others waiting in silence. No one had brought anything to read.
I did not know how to approach people: do some want to talk? Do some appreciate the silence? I took the plunge, despite the fact that it is pretty awkward being in a wheelchair and having my assistant driving me to each person directly.
I’d like to talk about three of the people who I gathered the nerve to approach.
First, an older woman across the room from me who smiled at me. I started out by asking when her appointment was, and if she had MS. She said that she was here for a consultation, because she was originally diagnosed with a nonspecific demyelinating disease. She was referred to the clinic by her primary care physician for a second opinion. She opened up to me, and was more than willing to share. We spoke briefly and then she left for her appointment.
The next person was a young gentleman, possibly in his late twenties, with his hands gently folded on his lap and his eyes half closed: he appeared to be meditating. I asked whether I could talk to him. I apologized for interrupting and asked him if he was meditating; he said he was. He proceeded to thank me profusely for noticing. I told him I had just started to explore meditation. We then spoke about what types of meditation he practices, and the new type of meditation that I am starting to practice. Then I took a big leap, and asked him how he is dealing with his MS. He told me he had progressive MS, and that he was trying to get used to his new life in a wheelchair. He thought that living with MS was hard – at times manageable and at other times, too much. He was very approachable, in fact, he was anxious to talk. I asked him, if we had the ability to record his story, would he be willing to participate? He said he would love it.
My third interaction was with a young woman nearby. We talked about MS, how we were dealing with it. We talked about family, pain, and medication. Everything seemed to flow so easily. Our conversation was warm and friendly – we exchanged information and agreed to talk again soon.
These brief interactions affirmed my belief that there is an untapped potential for connection in the waiting room.
The future of Waiting Rooms
I have always felt that it was lost time, a space where communication could happen. Now I want to start conversations with every single person waiting. I envision a waiting room culture where everyone feels acknowledged, and where patients and family members can talk about the struggles of living with illness together. My wish is that we all can learn from one another and feel more connected as a community.
The design of my most recent project was inspired in part by my experiences at Stanford Medicine X 2016. At the conference, it was a privilege to speak at length with Upali Nanda, an architect and designer who invites people to think about waiting rooms in a new way. She specializes in health care design and she encouraged me to work with her in envisioning clinical waiting rooms.
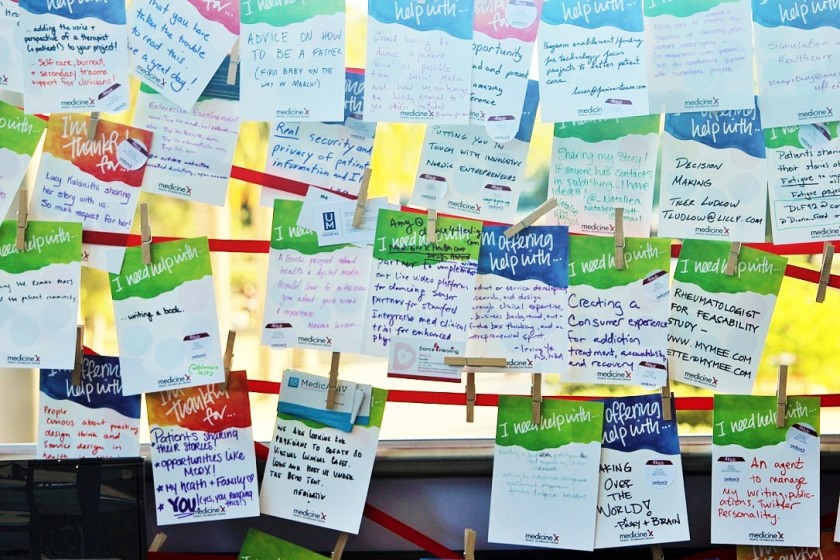
In addition to inspiration from my conversations with Upali, I also was inspired by an interactive space the folks at Medicine X created for attendees to share what they were thankful for, what they need help with, and what they can offer help with. People participated by writing their answers on large cards and displaying them. I utilize the idea of prompts on cards in my current project.
People respond to prompts at Medicine X 2016
Last weekend, I had the opportunity to test my ideas for interactive art in waiting rooms during an event put on by the MS Society. I was delighted to see people excited about the project, participating with enthusiasm.
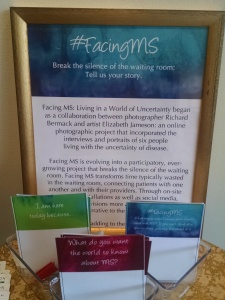
#FacingMS: an interactive installation using art and design to connect people
The following photographs depict my vision for interactive artwork that could truly “flip the wait.” Let’s transform the walls and the silence of the waiting room with installations like #FacingMS!
We had participants write a selected quote from their interviews directly on the artwork.
“The fear of the disease is the fear of the unknown. You could wake up and something else won’t work right.” – Will
“I do worry about the day I’m in a wheelchair. Walking doesn’t define me, but I feel bad for my partner, Paul.” – Mark
“I do not want to live smaller as a result of my diagnosis.” – Jessica
“You want to love your life, but you also can hate your life. It’s impossible not to feel overwhelmed.” – Elizabeth
“MS fatigue can feel like a wall coming down.” – Elsa
Three cards for three questions. “I am here today because…” “What do you want the world to know about MS?” and a blue #FacingMS card that has various unique, personal questions. In conjunction with our amazing experience at Medicine X (yet another inspiring experience from the conference) listening to Yoko K. Sen’s performance of Sound Will, we asked “What music would convey your experience with MS?”
Listen a song that embodies how MS can feel, through sound, for one person who attended the event.
Larry Chu, founder of Medicine X, giving his final remarks
During a time when technology is in the forefront of healthcare delivery and design, the question is what can technology do for patients, and how can healthcare providers tap into tech to better their practice?
As a patient seeking answers, I found some inspiration at Stanford Medicine X, a conference that explores how technology, social media and innovation can revolutionize and improve healthcare.
What an incredible mix of people at the conference. Medicine X is a thriving ecosystem of people from all disciplines, industries, and sectors. A unifying trait across the board was the sense of interconnected sharing – the fluidity of information, transparency of systems, and ease of connection.
At any given moment, I might have been in conversation with representatives from bio-pharmaceutical companies, architects, anesthesiologists, designers, social media strategists, marketing experts, innovation officers, health care providers, medical device manufacturers, genetic analysts, MBAs, radiologists, concerned citizens, entrepreneurs, PHDs, software developers, patients, clinicians, open-access researchers, holistic healers, strategy consultants, lawyers, nurses, principal user experience designer, project managers, investment analyst, bloggers, scientists, biomedical engineers, journalists, and yes, the list goes on.
While many of the people I met came from such vastly different backgrounds from me, I felt like I had equal footing with each and every attendee. I do not routinely mix with engineers, no less pharmaceutical representatives or high-tech people who thrive on quantitative analysis and “metrics.” I am an artist; I am comfortable brainstorming with designers, illustrators, eccentrics and activists. I was struck, however, by how often I found myself having a meaningful, free-flowing conversation with individuals from any and all sectors.
The experience was overwhelming and transformative.
“Patient-centered” – Medicine X talks the talk but can they walk the walk?
New friends at Med X! Ally, Thatcher, Nick, Danielle & me
Before I attended Medicine X, I was apprehensive. Much of the “Everyone Included” (ei) rhetoric sounded too good to be true. Patients running the game? In case you haven’t caught on in previous posts, I am a quadriplegic. Not many events are explicitly made accessible to me, and as a patient I must tirelessly self-advocate in places that are not patient-centered. The “ei” brand sounds fantastic, but I set the bar low in preparation for a weekend that would be more in line with my past experiences.
However, once I arrived at Medicine X it was clear that the lingo was not just phonics. The staff at Medicine X practice what they preach, and my caretaker and I were stunned by the sense of community that has been fostered among alumni who were in attendance. This community has grown in part out of the support and ease with which Medicine X includes the patient voice. Several of the talks we attended had a down up structure: patients generate ideas, and are major players in shaping the narrative. Med X is advertised as being the largest all-inclusive conference, meaning patients are at the forefront. For example, Karen Sandler, an executive with Software Freedom Conservancy, needed a defibrillator after a devastating encounter with heart disease changed the course of her work. She decided to refocus her work, providing pro bono legal assistance to people seeking information around the medical devices they were fit with.
New community
Yoko Sen, a sound artist I featured in my last post, performed at the conference. She was incredible! Read more about her mission to reinvent the sound environments of hospitals here.
In addition to the accessibility of the conference and the thoughtfulness of the staff, I was struck by how warm and supportive the other people who have illnesses were towards me. I made two new friends who have a very special place in my heart; several activists who survived brain tumors, and others who manage type 1 diabetes, and a mother of a child with heart disease. We all shared a common desire to reach out to other patients to strengthen community among people living with disease.
Social media has had a huge impact on me this year. I am now on Twitter and Instagram, I’ve established my own personal blog, and I’ve contributed to the Huffington Post. I was swept up by the momentum of Medicine X and the emphasis on technology & social media as a resource for community-building. These experiences fill me with the desire to become a fierce advocate and activist for those with imperfect bodies.
Conference highlights
Aside from the patient-centered nature of the conference and the vibrant community I have discovered both in person at #MedX and online, I wanted to address specific moments that stood out to me over the weekend.
Chronic Illness & Mental Health – I attended a workshop on chronic illness and mental health, where a panel of patients spoke about their experiences. I had the opportunity to meet each and every one of them throughout my time at the conference; their wisdom was inspiring. When we only seek help when trauma strikes; we are unprepared. Our mental health is not automatically present – rather it is a practice we must pay attention to every day. Someone on the panel likened it to swimming; if you haven’t learned to swim and are thrown into the water, you will not stay afloat. Just like swimming – if we don’t practice mental health on a day-to-day basis so that we have skills already formed, we will not have the resources for those tough moments often associated with chronic illness.
Radical Change-Makers – A seminar on radicals – people willing to challenge the status quo in a healthcare environment that resists change — where I learned that saying, “No,” is not a rejection of your good ideas, but a rite of passage. If you are trying to create systemic change, you are going to get knocked down again and again. Rejoice in the “Nos,” because with each one you are a step closer to a “Yes.” I enjoyed this lesson because I have repeatedly been denied the opportunity to implement innovative design strategies to improve patient experience in waiting rooms. I’ve gained a fresh perspective in that I now see the negative responses are a part of a lifetime commitment to dismantling conservative, traditional ways of providing healthcare.
Communication Strategies – In turn, faculty members from the business school lectured on effective communication strategies for negotiating change.
Storytelling Soundscapes – Lastly, the closing ceremony that featured an ambient electronic musician, Yoko K. Sen, was the perfect end to the conference. I featured Yoko in an earlier blog post; she is using her gifts as a sound artist to “a social enterprise to reimagine the sound environment in hospitals,” Yoko incorporated voices from people at the conference.
Inspiration
I am inspired to use art and design to further my mission to transform the narrative of illness, working to expand what it means to live in an imperfect body. I want people to see, hear, and connect with those of us with illness. I want people who have illness to engage their lives with dignity, to see themselves as a source of fascination, full of wisdom and grace.
As an artist who also spends a lot of time in the waiting room, I have often reflected on how time wasted in the waiting room could be utilized as a creative, productive, and healing time. I have written about the potential of the waiting room previously, and as I have continued to explore creative strategies for improving healthcare, sound art has captured my attention.
Sound design as a step towards creating patient-centered, humanized healthcare
As a visual artist, when I think about reshaping the waiting room experience for patients, I think about imagery. I think about the physical spaces people move through, and the tactile environment they might experience in a moment of vulnerability and stress. This week I came across Yoko Sen, an electronic musician, producer, engineer, vocalist and sound designer who expanded my thought process to include something invisible yet incredibly impactful in clinical settings: sound.
Yoko’s goal is to convert chaotic sounds of hospitals into more “soothing” soundscapes. She founded Sen Sound, “a social enterprise to reimagine the sound environment in hospitals.”
How do the sounds in hospitals impact our experience of illness?
After learning more about Sen Sound, I realized that I too have internalized the sounds of my hospital experience. As a person with Multiple Sclerosis, I’ve been in the hospital numerous times, having countless MRIs over the years to track the progression of my illness. Listening to the sounds of the MRI inspired me to create the following track several years ago, using sounds I found on the internet:
While I used the sounds I had to work with to try and process my own experience, Yoko and her company Sen Sound is doing something revolutionary. Their mission is to create “human-centered sound design to transform patient and staff experience.” They have conducted research with patients, family members and health care professionals to discover how the relentless noise of the hospital could become a harmonious, peaceful soundscape.
I am looking forward to seeing her perform at Medicine X, a health conference I will be attending in just two weeks. Yoko’s live performance will be of Sound Sen’s most current project, Sound Will, which focuses on the last sound people would like to hear instead of a chaotic blend of alarms, doors slamming, and hospital equipment. The project was one of top ideas selected by a recent Open IDEO challenge.
My current days are absolutely insane. You’d think I’d be winding down, with an artist practice as mature as mine, and the fact I don’t have use of my hands (I have MS and am a quadriplegic). Quite the opposite, though. My artist assistant Catherine Monahon and I have a lot going on.
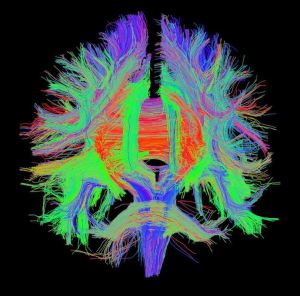
An example of one of my DTIs
In the middle of preparing for three upcoming shows and embroidering my next series on Diffusion Tensor Imaging(DTIs – a form of neuroimaging which tracks the flow of water through the brain, forming beautiful, interconnected, almost sculptural imagery), we decided, wouldn’t it be fun to start a blog. None of this would have happened without Catherine’s persistence. I mean… assistance.
What will I write about in this blog?
I will be using this blog to expand ideas focusing specifically on this intersection between the arts and healthcare. If you’ve had a chance to read my bio, you may already know that in addition to being an artist and a former lawyer, I’m also a patient. I will be featuring other artists who contribute to art and health, researching clinical settings that do patient-centered care well, and writing about various storytelling initiatives that catch my eye.
My “aha” moment came to me while I was waiting for one of my own neurology appointments. I was upset when I spent one hour waiting (by no means a new phenomenon), and the only thing remotely stimulating in the office was a huge television screen, on mute, projecting images of baby animals. I was offended. What, do they think we are all stupid? Baby animals at a Multiple Sclerosis clinic feels like a Band-Aid stuck on the forehead of a person who is facing a life-changing disease.
Powerful, real stories; not band-aids and smiley faces.
That hour, and all the hours that people spend sitting in waiting rooms, has potential. Potential to build community, to improve patient experience, and to reshape the way we interact in healthcare settings.
I am fascinated by the power of storytelling, and I know it has a place in the silence of the waiting room. I’m drawn to the StoryCorps model, and would like to create an art installation that will allow patients to share stories, listen to stories, and pose questions for other patients to consider. Stay tuned for developments on this.







 Tell us more about “Laughing Stock.”
Tell us more about “Laughing Stock.”

 The shared community and exchanges between people at Laughing Stock reveal that there are still opportunities in life, even if one lives with an illness. “It’s easy to feel like no one understands what your thinking, but then [during rehearsal, you try something] – everybody saw it, everybody gets it.” This unifying moment is transforming.
The shared community and exchanges between people at Laughing Stock reveal that there are still opportunities in life, even if one lives with an illness. “It’s easy to feel like no one understands what your thinking, but then [during rehearsal, you try something] – everybody saw it, everybody gets it.” This unifying moment is transforming.